
Quick Links:
For many Australian women, the journey to an endometriosis diagnosis begins with a feeling that something isn’t right.
Perhaps you’ve missed work because the pain was overwhelming. Maybe you’ve cancelled social plans, struggled through school or university, or found yourself curled up on the couch with a heat pack wondering how something that’s supposedly “just part of being a woman” can feel so debilitating. For years, many women have been told that painful periods are simply something to put up with and while some discomfort during menstruation can be normal, severe pain that interferes with your ability to work, study, exercise, socialise or enjoy everyday life is not.
For some women, that pain may be a sign of endometriosis. Endometriosis is a chronic condition that affects approximately one in nine Australian women by the age of 44 and is one of the most common causes of chronic pelvic pain in women of reproductive age. Despite how common it is, it remains widely misunderstood, underdiagnosed and, in many cases, dismissed.
At HIF, we believe informed health decisions start with reliable information. This article will help you understand endometriosis, recognise the symptoms and know when it may be time to speak with your GP.
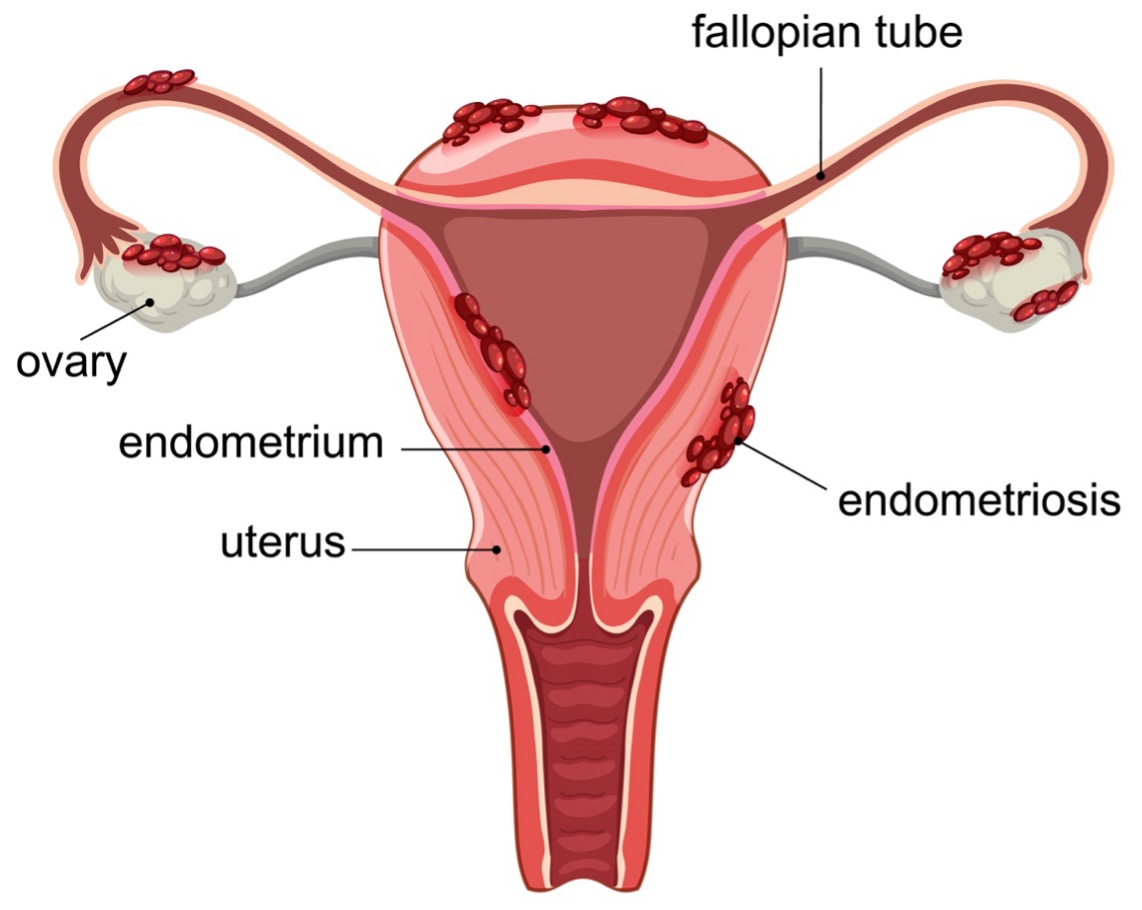
Figure 1. Medical illustration of endometriosis
To understand why endometriosis can have such a significant impact on daily life, it helps to first understand what is actually happening inside the body. Endometriosis is a chronic condition where tissue similar to the lining of the uterus, known as the endometrium, grows outside the uterus. These growths can occur on the ovaries, fallopian tubes, bladder, bowel and other structures within the pelvis. Like the tissue inside the uterus, this tissue responds to hormonal changes during the menstrual cycle. The difference is that it has nowhere to go when it breaks down. Over time, this can lead to inflammation, irritation, scarring and the formation of adhesions, where tissues and organs become stuck together.
Unlike a typical menstrual cycle, endometriosis involves ongoing inflammation that can continue beyond menstruation. This is one reason why many women experience pain throughout the month rather than only during their period. It’s also important to understand that endometriosis is not simply a heavy or painful period. While painful periods are one of the most common symptoms, endometriosis is a complex medical condition that can affect multiple areas of a person’s health and wellbeing. The condition most commonly affects women during their reproductive years and often begins during adolescence. Many women report experiencing symptoms for years before receiving a diagnosis.
The Australian Government has recognised the significant impact of the condition through its National Action Plan for Endometriosis, reflecting the growing understanding that endometriosis is a serious health issue that deserves greater awareness, research and support.
At HIF, we’re passionate about helping women take a proactive approach to their health. Our article on Essential Health Checks Every Woman Needs to Take Charge of Her Health highlights some of the preventative conversations and screenings that can help women stay informed about their wellbeing throughout every stage of life.

One of the challenges of endometriosis is that no two experiences are exactly alike. Some women with extensive endometriosis experience relatively mild symptoms, while others with less visible disease can experience debilitating pain.This can make recognising endometriosis particularly difficult and is one reason diagnosis often takes longer than it should.
Common symptoms of endometriosis include:
- Severe or debilitating period pain that may not improve with over-the-counter pain relief
- Chronic pelvic pain, including pain outside of menstruation
- Pain during or after sex
- Pain with bowel movements or urination, particularly around menstruation
- Heavy menstrual bleeding or irregular periods
- Bloating, nausea and fatigue, often referred to informally as “endo belly”
- Difficulty conceiving or fertility challenges
If you’ve ever felt that your symptoms have been dismissed or downplayed, you’re not alone. Many women living with endometriosis describe years of feeling unheard before finally receiving answers.
It’s also important to remember that not all pelvic pain is caused by endometriosis. Conditions such as adenomyosis, irritable bowel syndrome (IBS), interstitial cystitis and PMOS can present with similar symptoms. This is why self-diagnosis can be difficult and why professional assessment is so important.
For a detailed overview of symptoms, diagnosis and treatment pathways, Healthdirect’s endometriosis resource provides evidence-based information tailored to Australian patients.
Pelvic pain is one of the most common symptoms of endometriosis, but it’s not always limited to the menstrual cycle.
Because endometriosis involves inflammation, scar tissue and tissue growth outside the uterus, pain can occur before, during and after a period. Some women experience symptoms mainly around menstruation, while others live with ongoing pelvic pain throughout the month.
In some cases, endometriosis can affect nearby organs such as the bladder or bowel. Adhesions and scar tissue may cause tissues and organs to stick together, contributing to chronic discomfort. Ovarian cysts known as endometriomas can also develop and become a source of ongoing pain.
The experience of pain can vary significantly from person to person. For some women, symptoms may be manageable, while for others they can affect work, study, exercise, relationships and everyday activities.
If you’re experiencing persistent pelvic pain, it’s important to seek medical advice. While endometriosis is one possible cause, pelvic pain can also be associated with a range of other conditions that require different approaches to treatment. At HIF, we recognise that living with a chronic condition can affect both physical and emotional wellbeing. Our Mental Health Hub provides information and resources to help Australians better understand and support their overall health.
One of the challenges of endometriosis is that diagnosis can take time. Many women experience symptoms for years before receiving answers, partly because the condition can present differently from person to person.
The first step is usually a conversation with your GP. Keeping a record of your menstrual cycle, pain levels, bowel and bladder symptoms, and how they affect your daily life can provide valuable information during appointments.
Depending on your symptoms, your doctor may recommend investigations such as ultrasound or MRI imaging. While these tests can sometimes identify signs of endometriosis, particularly in more advanced cases, they cannot definitively confirm the condition.
At present, the gold standard for diagnosis remains a laparoscopy, a minimally invasive surgical procedure that allows a gynaecologist to directly view endometriosis tissue and, where appropriate, take biopsies.
Receiving a diagnosis can provide greater clarity about the cause of symptoms and help guide treatment and symptom management.
If specialist consultations or procedures become part of your healthcare journey, HIF members can learn more about eligible services through our information on gynaecology cover and the support available for a range of women’s health conditions. Endometriosis Australia also provides educational resources and patient support tools that can help women better understand the diagnosis process and advocate for their own care.
One of the biggest concerns many women have after being diagnosed with endometriosis is whether it will affect their ability to have children. While endometriosis can affect fertility, it’s important to know that a diagnosis does not automatically mean infertility.
Endometriosis may make conception more challenging due to inflammation, scar tissue, adhesions or ovarian endometriomas. However, many women with endometriosis conceive naturally and go on to have healthy pregnancies.
If you’re trying to conceive and have concerns about endometriosis, speaking with your GP or specialist is the best place to start. Early intervention and personalised advice can help identify the most appropriate pathway forward.
Some women find their symptoms improve during pregnancy due to hormonal changes that temporarily suppress the menstrual cycle, although symptoms often return after pregnancy.
It’s also important to remember that pelvic pain during pregnancy can have a range of causes and shouldn’t automatically be assumed to be related to endometriosis. Any pain experienced during pregnancy should be discussed with your healthcare provider.
For those who require additional fertility support, assisted reproductive technologies such as IVF may be recommended. HIF members can learn more about our Assisted Reproductive Technology cover and what support may be available for eligible members.
There is currently no cure for endometriosis, but there are a range of treatment options available that can help manage symptoms, reduce pain and improve quality of life.
Because every person’s experience of endometriosis is different, treatment plans are highly individualised and are typically developed in consultation with a GP, gynaecologist or multidisciplinary care team.
Pain Management
For many women, treatment begins with managing symptoms.
Non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, are often recommended to help reduce inflammation and relieve period pain. Depending on symptom severity, some women may also benefit from prescription medications or referral to a pain specialist.
The goal isn’t simply to mask symptoms. Effective pain management can help women maintain participation in work, study, exercise and daily life while longer-term treatment strategies are explored.
Hormonal Therapies
Hormonal treatments are among the most common approaches used to manage endometriosis symptoms.
These treatments aim to regulate or suppress the hormonal changes that trigger endometriosis activity and inflammation.
Options may include:
- The combined oral contraceptive pill
- Progestin-only medications
- Hormonal intrauterine devices (IUDs)
- Medications that reduce oestrogen production in more advanced cases
Many women experience significant symptom improvement through hormonal management, although treatment effectiveness varies from person to person.
Lifestyle and Supportive Therapies
If you’d rather not go down the hormonal treatment path, or you’re looking for ways to support your wellbeing alongside medical treatment, there are a range of lifestyle and complementary therapies that may help manage symptoms.
Approaches such as physiotherapy, yoga, cognitive behavioural therapy (CBT) and acupuncture are commonly used by women living with endometriosis. While more research is needed to fully understand their effectiveness, some women find these therapies help them manage pain and improve their quality of life.
Dietary changes may also play a role. Some women choose to increase foods rich in omega-3 fatty acids, such as oily fish, walnuts and flaxseeds, which are thought to support the body’s natural response to inflammation. Others explore supplements or herbal products such as ginger and turmeric, although evidence for their effectiveness in managing endometriosis symptoms is still emerging.
It’s important to remember that complementary therapies are not a substitute for medical treatment, and what works for one person may not work for another. If you’re considering supplements, herbal medicines or other natural therapies, speak with your GP or healthcare provider first, as some products can interact with prescribed medications.
Increasingly, a multidisciplinary approach that combines medical care with supportive therapies is recognised as an important part of helping women manage the physical and emotional impacts of endometriosis. At HIF we undertand the Importance of a holistic approach to healt and support members through our complimentary therapies cover.
Endometriosis Surgery
For some women, surgery forms an important part of treatment.
Laparoscopy remains both the gold standard for diagnosis and the primary surgical treatment for endometriosis. During the procedure, a gynaecologist can identify, remove or excise endometriosis lesions and scar tissue.
While surgery can provide significant symptom relief and may improve fertility outcomes for some women, it’s important to understand that surgery is not considered a permanent cure. Endometriosis can recur, which is why ongoing management is often recommended after surgical treatment.
HIF members can explore our information on gynaecology services and cover to better understand what support may be available if surgery becomes part of their treatment plan.
For many years, conditions such as endometriosis received relatively little public attention despite affecting millions of women worldwide. Today, that is beginning to change. Endometriosis has become one of the leading examples of why women’s health deserves greater attention. Despite affecting around one in nine Australian women by age 44, the condition has historically been under-recognised, underfunded and poorly understood.
Research published in Nature highlighted that several conditions affecting women remain significantly underfunded relative to the burden they place on individuals and healthcare systems. Women have also historically been underrepresented in clinical trials, creating gaps in our understanding of how certain conditions present, progress and respond to treatment.
The encouraging news is that awareness, advocacy and investment in women’s health are growing. Australia became one of the first countries in the world to introduce a dedicated National Action Plan for Endometriosis, helping drive improvements in education, diagnosis and clinical care. According to the World Economic Forum, governments, researchers and healthcare organisations are also placing greater focus on closing long-standing gaps in women’s healthcare outcomes.
Growing recognition of women’s health issues can also be seen in the recent renaming of polycystic ovary syndrome (PCOS) to polyendocrine metabolic ovarian syndrome (PMOS). Published in The Lancet, the change reflects efforts to improve understanding of conditions that affect women and ensure medical terminology better reflects the complexity of these conditions.
While there is still progress to be made, there are genuine reasons for optimism. More women are speaking openly about their experiences, healthcare professionals are becoming better equipped to recognise symptoms earlier, and research into endometriosis and women’s health continues to gain momentum.
Living with endometriosis can be challenging in ways that aren’t always visible to other people. Pain is only one part of the story.
For many women, endometriosis affects work, study, relationships, exercise, social plans and mental wellbeing. Symptoms can be unpredictable, making it difficult to commit to activities with confidence. Even on good days, there can be uncertainty about when symptoms might flare again.That uncertainty can be exhausting and it’s also why support matters so much.
Whether it’s a trusted GP, specialist, physiotherapist, partner, family member or support group, having people who understand what you’re experiencing can make a significant difference. Organisations such as Endometriosis Australia and Jean Hailes for Women’s Health provide valuable information, educational resources and support for women navigating life with the condition.
Many women also find benefit in strategies that complement their medical treatment plan, including:
- Gentle movement and regular physical activity
- Heat therapy during symptom flare-ups
- Prioritising sleep and recovery
- Stress management techniques
- Dietary approaches guided by qualified healthcare professionals
At HIF, we believe health is about more than treating illness. It’s about supporting wellbeing in a way that fits real life.
That’s why we provide resources through our Healthy Lifestyle Hub and offer access to a range of Health and Wellbeing Programs designed to support members in taking a proactive approach to their overall health.
Perhaps most importantly, we encourage women to trust their instincts.
If something doesn’t feel right, keep asking questions. Track your symptoms. Bring notes to appointments. Seek a second opinion if needed. You know your body better than anyone else.
Endometriosis is common, complex and often misunderstood. It affects millions of women worldwide and approximately one in nine Australian women by age 44. Yet despite how common it is, many women still spend years searching for answers before receiving a diagnosis.
The good news is that awareness is growing, treatment options continue to improve, and conversations about women’s health are becoming more open than ever before.
The most important message is simple: severe pain is not something you should have to simply endure.
If painful periods, pelvic pain or other symptoms are affecting your ability to work, study, exercise or enjoy everyday life, it’s worth speaking with your GP. Early conversations can lead to earlier diagnosis, earlier treatment and better long-term outcomes.
At HIF, we’re proud to support Australian women through every stage of life. Whether that means providing trusted health information, helping members understand their cover options, supporting access to gynaecological care or assisting eligible members with fertility treatment, we’re committed to helping Australians make informed decisions about their health and wellbeing.
What is endometriosis?
Endometriosis is a chronic condition where tissue similar to the lining of the uterus grows outside the uterus. This tissue can cause inflammation, scarring, pelvic pain and, in some cases, fertility challenges.
What are the symptoms of endometriosis?
Common symptoms include painful periods, chronic pelvic pain, pain during or after sex, heavy menstrual bleeding, bloating, fatigue, pain with bowel movements or urination, and difficulty conceiving. Symptoms can vary significantly between individuals.
How is endometriosis diagnosed in Australia?
The only definitive way to diagnose endometriosis is through laparoscopy, a minimally invasive surgical procedure that allows a gynaecologist to directly examine and biopsy affected tissue. Imaging such as ultrasound and MRI can assist assessment but cannot confirm the diagnosis on their own.
Why does endometriosis take so long to diagnose?
Symptoms are often normalised, mistaken for other conditions or dismissed as severe period pain. As a result, many Australian women experience significant delays between symptom onset and diagnosis.
What are the treatment options for endometriosis?
Treatment options may include pain relief medications, hormonal therapies, surgery, physiotherapy, psychological support and fertility treatments. The most appropriate approach depends on an individual’s symptoms, goals and overall health.
Does endometriosis affect fertility?
It can affect fertility in some women, particularly when inflammation, adhesions or ovarian involvement interfere with normal reproductive function. However, many women with endometriosis conceive naturally and have healthy pregnancies.
What is PMOS and how does it relate to endometriosis?
PMOS, or polyendocrine metabolic ovarian syndrome, is the new name for PCOS. While PMOS and endometriosis are separate conditions, they can share overlapping symptoms such as pelvic pain and menstrual irregularities, which sometimes contributes to delayed diagnosis.
Can I get support through my HIF cover?
Eligible HIF members may have access to cover for gynaecological procedures, including treatments related to endometriosis. Assisted reproductive technology cover may also be available for eligible members seeking fertility support.
Where can I find more information about endometriosis in Australia?
Trusted Australian sources include Endometriosis Australia, Healthdirect, Jean Hailes for Women’s Health and the Australian Government’s National Action Plan for Endometriosis. HIF members can also explore additional information through the HIF Health Hub.